
{kind=link}
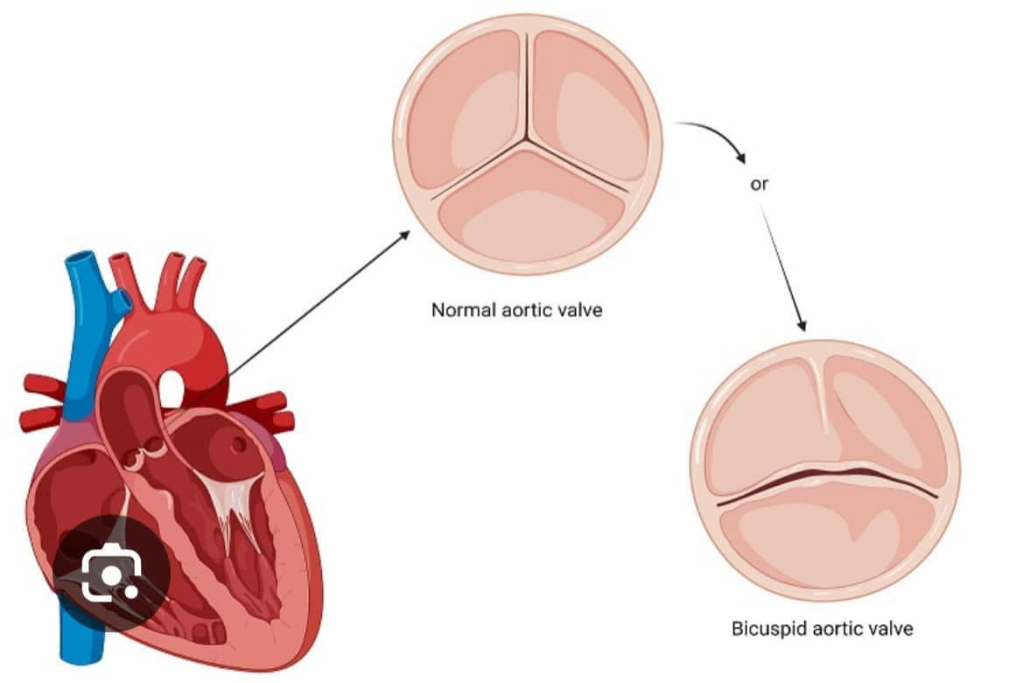
One to two percent of the general population have bicuspid aortic valves (BAV).
Although a BAV may remain without clinical consequences for a lifetime, it can deteriorate into aortic valve stenosis and regurgitation and aortic dilatation/aneurysm.
According to our recent interview with Dr. Patrick Vargo of Cleveland Clinic, ascending aortic aneurysms in people with BAV tend not to extend beyond the beginning of the aortic arch.
The consensus, including current international guidelines, is that athletes with BAV with normal valvular function and no aortic dilation can participate in all athletic activities.
A December, 2024 clinical study of 407 people with BAV over their lifetimes confirmed no negative associations between exercise volumes or intensity or sport type and valve dysfunction or aneurysm growth.
In that study, 133 people were sedentary (<500 metabolic equivalent of task minutes per week). 94 were active (500–1000 metabolic equivalent of task minutes per week), and 180 highly active (≥1000 metabolic equivalent of task minutes per week).
In fact, the study concluded that participation in vigorous intensity exercise was associated with lower risks of aortic stenosis.
Still, those with mild aortic dilation should undergo annual screening, some more frequently than others.
Those with moderate or severe valvular stenosis or regurgitation should be managed based on the hemodynamic impact of the valve lesion, a procedure that checks blood circulation and evaluates how well the heart is working.
Athletes with lesions and/or syndromes such as Marfan should be evaluated comprehensively before exercise.
Individuals with severe aortic regurgitation may participate in low- and moderate-intensity exercise if the left ventricular is not dilated, the left ventricular ejection fraction remains more than 50%, the aortic root is within normal dimensions or is mildly dilated, and exercise stress testing results are normal.
Only low-intensity exercise is recommended for those with a dilated left ventricle, a left ventricular ejection fraction of less than 50%, significant aortic root dilatation, or exercise-induced arrhythmias.
In other words, for people with BAV, it’s complicated and exercising requires consultation with your cardiologist.
What counsel have you received from your doctor on BAV and exercise?
For a deep dive:
December 2024 study
https://www.ahajournals.org/doi/10.1161/JAHA.123.031850
For general info on BAV and exercise see:
https://academic.oup.com/esc/book/40438/chapter-abstract/347533926?redirectedFrom=fulltext#
For a study on an elite endurance triathlete with BAV complications see:
https://www.jacc.org/doi/10.1016/j.jaccas.2022.05.021
For information on hemodynamic monitoring:
For information on aortic dilation, see: